


On Feb 9, 2024, media reported on a passenger who died during a Lufthansa flight from Thailand to Germany on Feb 8, 2024. Eyewitness reports provided the following facts:
• 63 years old male.
• Passenger was ill-appearing even before boarding the airplane.
• Profuse bleeding occurred from the nose and mouth.
• Litres of blood was lost with splattering to the walls of the airplane.
• Flight attendants tried to resuscitate the passenger for 30 minutes before he died.
There are only a few things I can think of to explain what happened. starting with the most to the least likely.

1) A very bad nosebleed. Not the typical one that most people get (anterior nosebleed), but one that occurs from the sphenopalatine artery (posterior nosebleed). There is a fairly large artery located in the very back of the nose which can rarely erupt causing a very bad nosebleed that typically occurs out the nose and mouth. Without bleeding control which mandates posterior nasal packing, it is entirely conceivable that death would occur within 30 minutes. Blood hitting the wall may be due to coughing as blood drips into the throat unexpectedly. However, one does not have to be ill to suffer from such nosebleeds.
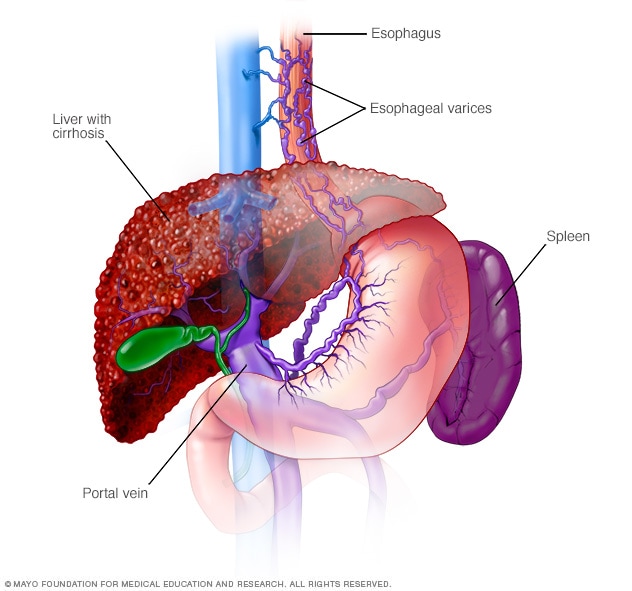
2) Esophageal varices rupture. Esophageal varices develop when regular blood flow to the liver is blocked by a clot or scar tissue in the liver. To go around the blockages, blood flows into smaller blood vessels that aren't designed to carry large volumes of blood. The vessels can leak blood or even burst, causing life-threatening bleeding, conceivably resulting in death in about 30 minutes. Such bleeding can be so copious that not only will the blood drain into the stomach, but also up and out the mouth and nose. Such patients are ill-appearing at baseline. This condition is treated by a GI specialist.
3) Carotid blowout. Passenger was ill-appearing which may have been due to a history of late-stage throat cancer that was treated with radiation therapy. In such cases, sometimes, the wall separating the carotid artery from the inside of the throat can be very thin. So thin, that it may rupture causing blood to suddenly pour out of the mouth like a geyser. The amount of bleeding can be so vigorous, it will also come out the nose and even eject out the mouth. Patients who suffer from a carotid blowout will usually die within minutes... not 30 minutes later, unless the carotid blowout is pinhole with ball-valving from surrounding soft tissues.
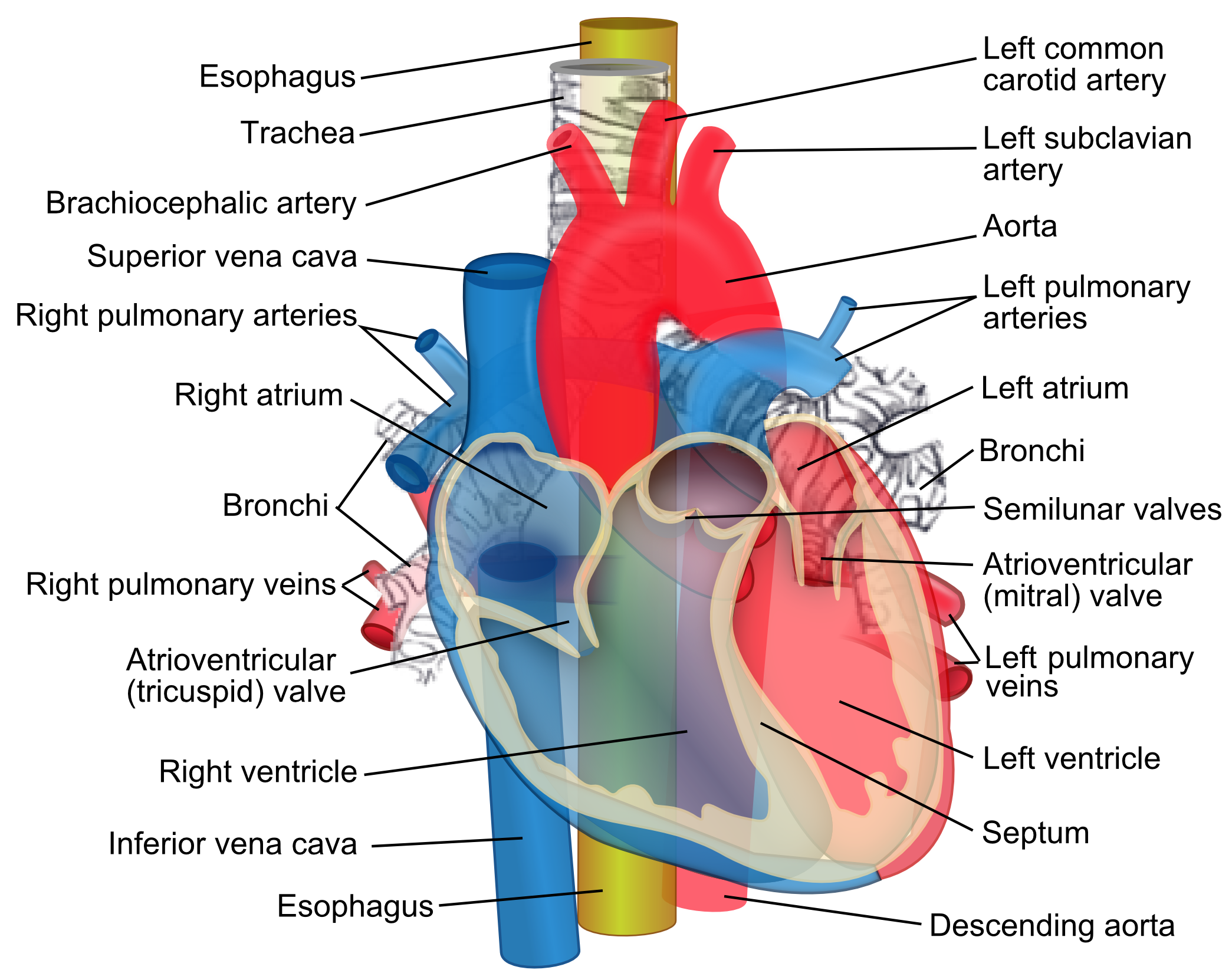
4) Tracheoinnominate fistula. Passenger was ill-appearing which may be due to a history of a tracheostomy due to prolonged intubation from respiratory failure. Obviously recovered enough to travel... and perhaps even no longer having a tracheostomy tube. With such a fistula, the aortic artery ruptures into the windpipe over a weakened area where the trach tube rubbed against the anterior tracheal wall. Similar to the carotid blowout, the amount of bleeding can be vigorous and since blood would be pouring into the windpipe, the patient would be literally drowning in his own blood. Coughing would occur to the point it would come out the nose and mouth. Patients who suffer from a tracheoinnominate fistula usually die within minutes. Certainly not 30 minutes later... but who knows? Maybe it was a very tiny pinhole fistula.
In the end, without more details, it is impossible to say what caused this passenger's death. No matter what the cause, without the ability to intubate to protect the airway and having the right tools immediately on hand, I'm not sure what even an ENT doctor would have been able to do to save this passenger's life in an airplane using only the on-board emergency medical kit.
At this time, the following items can be found in a FAA approved emergency medical kit.

No comments:
CLICK to Post a Comment